Open and endovascular treatment of abdominal angina
Abdominal (or intestinal) angina refers to a chronic circulatory disorder of the intestinal wall (chronic mesenteric ischemia). It is an early symptom and a warning sign of impending occlusion of a vessel supplying the intestine.
Overview
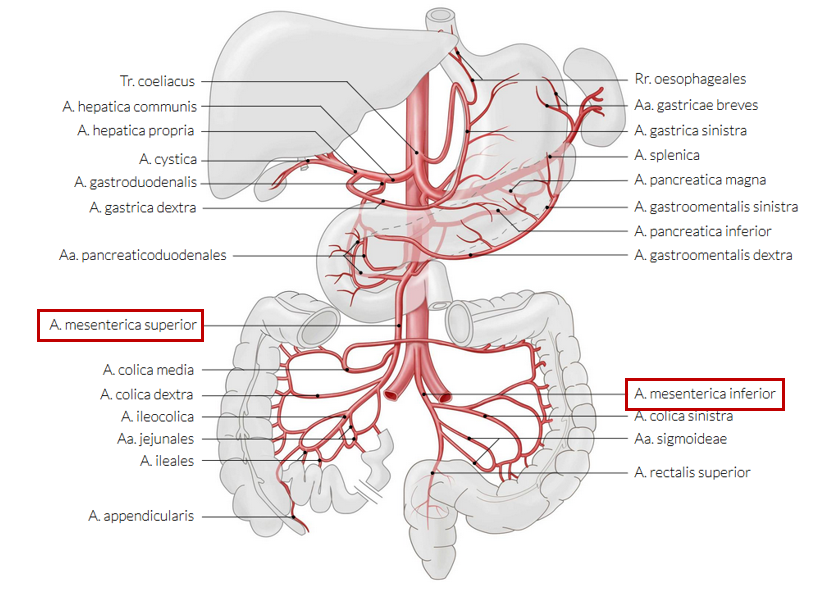
It usually occurs about 20-30 minutes after food intake and lasts about one to two hours, with pain being dull or sharp in character. The stomach and intestinal walls stretch after food intake, thereby compromising vessels, which further increases resistance to blood flow. This in turn leads to reduced blood flow and attacks of abdominal pain. . The commonest cause is atherosclerosis of the mesenteric vessels (superior and inferior mesenteric arteries) Risk factors thus also include those of atherosclerosis:
Smoking
High blood pressure
High blood fats
Family history
Clinical course
Imaging of the intestinal vessels is necessary if a chronic circulatory disorder is suspected. Doppler ultrasonography is typically the modality of first choice. Detailed assessment by computed tomography is then performed if a circulatory disorder is confirmed. Magnetic resonance tomography is an alternative imaging modality. The findings are discussed by an interdisciplinary team and a treatment plan proposed to the patient.
Open (surgical) treatment
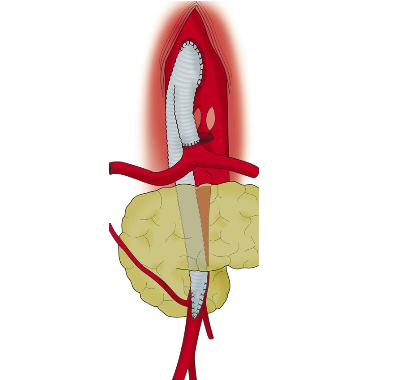
The aorta and involved vessels are exposed by an abdominal incision, followed by an appropriate operative intervention: Relocation of the vessel (re-implantation / transplantation), creation of an antegrade or retrograde bypass, reconstruction using a prosthesis (see image) or removal of calcium deposits (thrombendarterectomy) with vasodilatation (patch repair)
Endovascular treatment
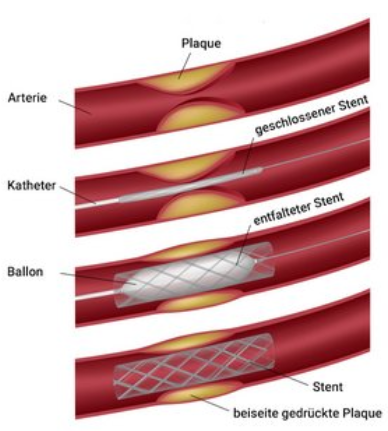
A catheter is introduced in to the vessel through a small puncture and the narrow segment is then dilated by means of a balloon. Professional associations currently recommend stent implantation in addition. Should treatment be necessary, the patient’s situation and the outcomes of various methods should be compared: Open surgery has better long-term results overall, while catheter-guided interventions are beneficial in the short-term. Open surgery should therefore be recommended for younger and otherwise healthy patients, while catheter-guided interventions may be considered in older patients with severe comorbidities. Both methods complement may one another in many cases.
Jimenez et al J Vasc Surg 2002
Alila Medical Media / fotolia
Preparation
Special preparation by the patient is not feasible. Treatment of risk factors (e.g., smoking, high blood pressure, etc.) is necessary during and after therapy.
Aftercare
Aftercare depends on the selected therapeutic option (open surgery versus catheter-guided treatment), and may be organized in a special rehabilitation clinic after treatment, if desired. Regular consultations are furthermore arranged in the vascular surgery outpatient department for monitoring of therapeutic outcomes. A change and modification of medication is necessary depending on the procedure performed.
Various procedures at the University Hospital Zurich
Treatment at the University Hospital Zurich offers various advantages. All known and modern treatment methods are available, as are combinations of two methods (hybrid methods) for suitable patients (e.g., ROMS Retrograde open mesenteric stenting). Patients with comorbidities also benefit from the interdisciplinary teamwork of the 43 departments of the University Hospital Zurich.
For patients
Register directly with the Clinic for Vascular Surgery for your first appointment.